Treatment
Ovarian Cancer
Ovarian cancer is a malignant tumor that originates in the ovaries, the female reproductive glands responsible for producing eggs and hormones. It involves the uncontrolled growth and multiplication of abnormal cells in the ovarian tissue, which can invade and destroy healthy tissue.
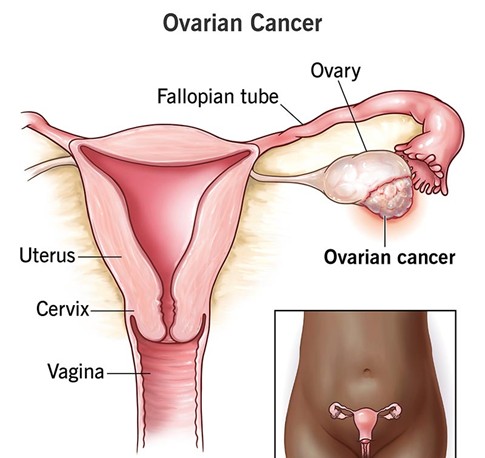
Types of Ovarian Cancer
The most common type is epithelial ovarian cancer, which begins in the cells covering the ovary and accounts for over 95% of cases. Related cancers include fallopian tube cancer and primary peritoneal cancer, which have similar origins and treatments and are sometimes grouped with ovarian cancer. Other less common types include malignant germ cell tumors and stromal tumors.
Within epithelial ovarian cancers, there are several subtypes:
- High-grade serous carcinoma (HGSC): The most common subtype, often originating in the fallopian tubes, accounting for about 75% of epithelial cases. It is aggressive and frequently diagnosed at an advanced stage.
- Clear-cell carcinoma: A rarer subtype linked to endometriosis, more common in younger women, especially of Asian descent. It tends to be resistant to chemotherapy.
Causes and Risk Factors
Ovarian cancer arises due to genetic mutations in the DNA of ovarian cells. These mutations may be acquired during a person’s lifetime or inherited. Inherited mutations in genes such as BRCA1and BRCA2 significantly increase the risk of ovarian and breast cancers. About 10% of ovarian cancers are hereditary.
Other risk factors include age (most cases occur after menopause), reproductive history (never having children or late childbirth), hormone therapy, obesity, endometriosis and family history of breast or ovarian cancer.
Symptoms
Early-stage ovarian cancer often causes no or vague symptoms, making early diagnosis challenging. As the disease progresses, symptoms may include:
- Pelvic or abdominal pain or pressure
- Bloating and abdominal swelling
- Changes in bowel habits (constipation)
- Frequent or urgent urination
- Unexpected vaginal bleeding
- Feeling full quickly when eating
- Fatigue, nausea, and weight loss
These symptoms can mimic other common conditions but tend to persist or worsen over time.
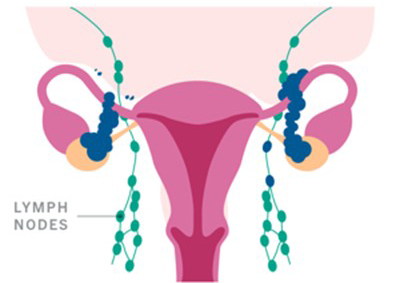
Spread of ovarian cancer
If ovarian cancer spreads, it usually does so from your pelvis to your lymph nodes, abdomen, intestines, stomach, chest or liver.
Diagnosis
Despite years of research, experts haven’t yet developed a successful ovarian cancer screening test. For this reason, the condition is often difficult to diagnose in the early stages.
If your doctor suspects ovarian cancer, they’ll ask about your symptoms and perform a pelvic exam. During the exam, they’ll check for any abnormal growths or enlarged organs.
They may recommend additional tests, including:
Blood tests
Blood tests includes CA-125 – is a protein present in blood which is usually raised, However, CA-125 levels can be normal, even when cancer is present, and higher in many conditions that aren’t cancer like endometriosis, PID, fever, during menstruation. The Ca-125 levels are used in combination with other tests to diagnose ovarian cancer and later it is used as a prognosticator.
An FNA or diagnostic paracentesis should be performed in patients with diffuse carcinomatosis or ascites without an obvious ovarian mass.
Surgical evaluation- Frozen section
Imaging studies
Imaging studies to consider, when clinically indicated, in patients with a presentation suspicious for ovarian cancer may include the following :
Pelvic ultrasonography
Pelvic and abdominal computed tomography (CT) scanning
Pelvic and abdominal magnetic resonance imaging: Increases specificity of imaging when sonography findings are indeterminate
Chest radiography: Routine imaging to exclude lung metastases; chest CT preferred if there is particular concern for metastatic or disseminated disease
Mammography: Part of preoperative workup for women older than 40 years who have not had one in the preceding 6-12 months; estrogen-producing tumors may increase the risk of breast malignancies, and breast cancers can metastasize to the ovaries and are often bilateral
Endoscopies
In patients with diffuse carcinomatosis and GI symptoms, a GI tract workup may be indicated, including one of the following imaging studies:
Upper and/or lower endoscopy
Barium enema
Upper GI series
Treatment
Ovarian cancer treatment typically involves a combination of approaches tailored to the
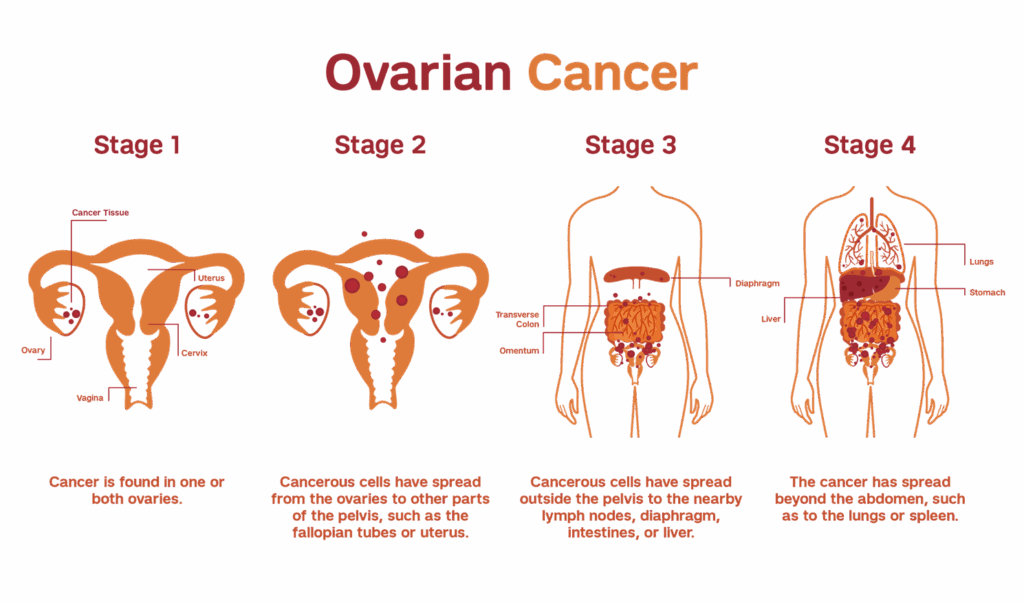
- Stage
- Type
- Spread
- Patient’s overall health.
The main treatments are surgery and chemotherapy, with additional options including targeted therapy, hormone therapy, immunotherapy, and supportive care.
Surgery
Surgery is often the primary treatment and varies depending on cancer extent:
- Early-stage cancer (confined to one ovary): Removal of the affected ovary and fallopian tube, potentially preserving fertility.
- Cancer in both ovaries without spread: Removal of both ovaries and fallopian tubes, sometimes preserving the uterus to allow future pregnancy with assisted reproductive techniques.
- More extensive cancer or no desire for fertility preservation: Removal of both ovaries, fallopian tubes, uterus, nearby lymph nodes, and fatty tissue in the abdomen (omentectomy).
- Advanced cancer: Surgery aims to remove as much tumor as possible (debulking). Chemotherapy may be given before or after surgery to shrink tumors or kill residual cancer cells.
Chemotherapy
Chemotherapy uses drugs to kill rapidly dividing cancer cells and can be administered:
- Before surgery (neoadjuvant) to shrink tumors.
- After surgery (adjuvant) to eliminate remaining cancer cells.
- As the main treatment if surgery is not possible or for recurrent cancer.
Drugs can be given intravenously, orally, or directly into the abdominal cavity (intraperitoneal chemotherapy). Heated chemotherapy infused into the abdomen during surgery (hyperthermic intraperitoneal chemotherapy) is another approach in certain cases.
Targeted Therapy
Targeted therapies attack specific weaknesses in cancer cells:
- PARP inhibitors (e.g., olaparib) block DNA repair in cancer cells, particularly effective in tumors with BRCA gene mutations.
- Monoclonal antibodies (e.g., bevacizumab) inhibit blood vessel growth that tumors need.
- Newer agents like mirvetuximab soravtansine target folate receptors common in ovarian cancer cells and show promising results for recurrent disease.
These therapies may be part of first-line treatment or used for recurrent cancer.
Hormone Therapy
Some ovarian cancers depend on estrogen to grow. Hormone therapy blocks estrogen effects and may be used for slow-growing cancers or if cancer recurs after initial treatment. This option is less common but can be effective in select cases.
Immunotherapy
Immunotherapy helps the immune system recognize and attack cancer cells that evade immune detection.
Drugs like immune checkpoint inhibitors (e.g., pembrolizumab) are sometimes combined with vaccines designed to boost immune response against ovarian cancer. Immunotherapy is generally considered in specific situations or clinical trials.
Radiotherapy
Radiation therapy is less commonly used but may help control symptoms or treat advanced cancer when other treatments are unsuitable.
Supportive (Palliative) Care
Palliative care focuses on relieving symptoms and improving quality of life during and after cancer treatment. It can be provided alongside curative treatments or when cancer is advanced
Prognosis
Ovarian cancer is the fifth leading cause of cancer deaths among women, with a 5-year survival rate of about 46%. Survival is better when the tumor is detected early and optimally resected, but most cases are diagnosed at an advanced stage due to the subtlety of early symptoms.
In summary, ovarian cancer is a serious and often late-diagnosed malignancy of the female reproductive system with several subtypes and risk factors. Early detection remains difficult, but advances in surgery and chemotherapy have improved outcomes for many patients. Genetic factors play a significant role, highlighting the importance of family history and genetic counselling in at-risk individuals.